
Utilizing Community-Based Approaches: Addressing Medical Non-Adherence in Black Hypertensive Patients

Introduction
Today, nearly 50% of adult Americans suffer from hypertension (Chobufo et al. 2020). Hypertension (HTN or high blood pressure) is the biggest risk factor for cardiovascular diseases worldwide. However, African Americans are disproportionately impacted by hypertension and its health outcomes compared to their white counterparts. Existing literature highlights the correlation between medical mistrust and medical adherence in Black patients. However, few studies have focused on how to address the underlying determinants of medical nonadherence in Black hypertension patients. To address the high prevalence of medical mistrust and its impacts on medical adherence in Black hypertensive patients, policymakers must address the systemic structures that contribute to perceived racism, unsafe environments, and stigma in healthcare.
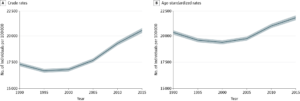
According to the World Health Organization, 1.28 billion adults live with hypertension. In the United States, nearly 50% of adults suffer from hypertension (Chobufo et al. 2020). Hypertension (HTN) or high blood pressure is a health condition that describes a consistently elevated blood pressure level. High blood pressure is a major risk factor for cardiovascular disease, stroke, and other cardiovascular-related illnesses. In addition to being a large risk factor for illness, HTN is a leading cause of premature death globally (WHO 2024).
While hypertension is highly treatable, nearly half of all adults with high blood pressure are aware of their condition. Further compounded by low rates of diagnosis, only 1 in 5 adults with hypertension manage their condition (WHO 2024). Uncontrolled hypertension greatly increases the risk of developing serious or chronic illnesses and mortality.
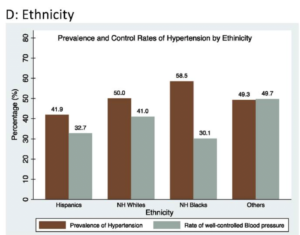
With the rise of modern medicine in the 20th century, the world saw a shift from a high prevalence of infectious diseases to non-communicable diseases (NCDs). This epidemiological transition was accelerated by globalization following the Cold War. Factors such as the internet and increased communication methods worked with neoliberal economic policies, shifting consumer preferences and patterns (Magnusson and Gostin 2023). Global health faced significant consequences due to McDonaldization, which replaced traditional food cultures with cheaper and more processed imports containing higher levels of fat, sugar, and salt. The digital age initiated a shift to more sedentary lifestyles, which compounded the impacts of poor diet (Magnusson and Gostin 2023). The epidemiological transition of the late 80s and early 90s reflected an increase in high blood pressure rates through the 2000s and 2010s. (Forouzanfar et al. 2017). While the rising prevalence of hypertension is a global problem, impacting over 1 billion adults, African-American adults have the highest prevalence of high blood pressure worldwide. In the United States, 55% of Black adults have hypertension, are more likely to have uncontrolled blood pressure, and have higher rates of severe hypertension than white adults (AHA 2024). Black Americans had higher rates of uncontrolled blood pressure than whites, 27% compared to 17% (Fuchs 2011).
The higher prevalence of hypertension in Black Americans than in White Americans highlights both structural and societal inequalities in America today. Researchers theorize that environmental and behavioral factors cause disparities in hypertension prevalence between Black people living in the United States and Africa. Studies found that African-American adults had a higher prevalence of high blood pressure than other members of the African Diaspora, disproving theories of genetic predisposition of Black populations. This difference between members of the African diaspora also highlights the structural causes of hypertension in the United States. Contributing factors to high blood pressure in African-American adults include “socioeconomic status, dietary habits, social network, stress, and health behaviors” (Fuchs 2011).
Racial disparities in hypertension management, a major risk factor for stroke and heart disease, contribute to approximately 8,000 preventable deaths in Black patients (Fiscella and Holt 2008). The gap in cardiovascular disease mortality rates and the unequal burden of HTN on Black Americans remains stagnant (Ferdinand et al. 2020).
Medical Adherence
Medical adherence is “the extent to which a patient adheres to the prescribed dose and interval of their medication regimen” (Brown et al. 2016). When a patient misses 80% or more of their prescribed daily dose, they are considered nonadherent. Patients are nonadherent to their medicine 50% of the time; however, for hypertension, nearly 80% of patients are nonadherent. There are many causes for nonadherence, but most are rooted in the patient-provider relationship. Understanding and trust are critical predictors of a patient’s adherence. These predictors appear in patient fears and emotional barriers to care. Due to the power imbalance in the patient-provider relationship, in which the provider has more knowledge, power, and education, many patients fear being admonished for nonadherence. Most patients do not reveal nonadherence to their providers, exacerbated by negative experiences with providers.
A study analyzing African Americans’ health beliefs investigated perceptions of patient-provider relationships. Patients who were adherent described physicians using phrases like: “caring,” “trustworthy,” and “reachable.” In stark contrast, nonadherent patients described providers as“noncaring,” “fear-inducing,” and noncompliant. Nonadherent patients also perceived physicians as prejudiced towards them based on their ethnicity (Lukoschek 2003).
Since trust is a large predictor of medical adherence, the concept of medical mistrust remains prevalent. Medical mistrust is “the lack of trust in or suspicion of medical organizations” (Powell et al. 2018). Mistrust increases rates of nonadherence, delays in seeking care, and lower appointment attendance. The determinants of mistrust are conflicting medical information, increased access to medical information, low continuity of care with personal physicians, medical errors, and malpractice (Powell et al. 2018). Medical mistrust is amplified for Black patients. Many studies have identified racism, particularly the Tuskegee Syphilis Study, as a root cause of medical mistrust in Black patients. Perceived racism in healthcare works in tandem with medical mistrust, and as a result, Black patients have reported higher negative health outcomes (Powell et al. 2018).
Trust in the patient-provider relationship goes both ways. Trustworthy physicians must prioritize the patient, communicate well, and display competency and goodwill. Patients must be honest, adhere to treatment, and make good health decisions (Abel and Efird 2013). Medical environments are stressful for many individuals; therefore, it is important to create a safe environment for patients. To encourage medical adherence, “a consistently blame-free environment” is necessary (Brown et al. 2016). Patients who experience mistrust are less likely to reveal nonadherence when healthcare teams are not empathetic. Providers must be careful when reacting to patient nonadherence and utilize neutral language to ensure that patients feel safe with them (Brown et al. 2016).
Stigma is the negative stereotyping and perceptions surrounding a particular attribute. The negative stereotypes contribute to the separation of ‘us versus them.’ Labeled persons experience discrimination and loss of social status. The negative stigma surrounding hypertension deeply impacts how the illness is perceived by patients and providers (Link and Phelan 2001). Additionally, social and self-stigma exacerbate medical nonadherence in hypertensive patients.
Due to the high rates of medical mistrust and nonadherence in Black patients, many researchers have conducted qualitative studies highlighting the patient experience. One study identified several themes in hypertensive patients’ perceptions of their condition. Participants who held a stigma towards hypertension were asked to express their feelings about their condition.
Qualitative Impacts on Patient Experience (Abel et al. 2021)
1) Shame and embarrassment
a) Themes
● Participants were embarrassed by taking medication in public, which may increase nonadherence.
● Experienced feelings of shame, failure, and discouragement because they felt they were not in control of their health.
b) Participant Responses:
● “I feel shame because it shows poor health. I don’t take care of myself like I should.”
● “Ashamed that I didn’t do all I could to prevent high blood pressure before it happened.”
● “[HTN is] embarrassing to talk about.”
2) Stereotype Threat
a) Themes
● A stereotype threat is “the threat of being viewed through the lens of a negative stereotype, or the fear of doing something that would inadvertently confirm that stereotype.” In hypertension treatment, participants largely believed that stigma impacts how others perceive them.
b) Participant Responses
● “I was [asked] to change my diet, especially salt, because I’m African American.”
● “I feel like people assume you don’t care about your health, you are lazy, uneducated, in poverty, never attempt to do better at taking care of yourself.”
3) Disrupted Normality
a) Themes
● For hypertensive patients, diagnosis is followed by a strict medication regimen and significant lifestyle changes, such as diet and exercise. The sudden shift is often seen as an unwanted burden to patients, leading to increased nonadherence.
b) Participant Responses
● “Yet another hindrance, where others have to consider or make provisions for me when we plan things together.”
What is Stress Process Theory?
In addition to the perceived racism in healthcare, there is significant evidence that racial and ethnic discrimination is a risk factor for high blood pressure (Brown et al. 2016). According to Leonard Pearlin, the stress process outlines how circumstances lead to stressful experiences. Stressful experiences can be divided into two categories: life events and life strains. Life events are discrete or acute events; those that are undesired, unscheduled, or uncontrolled are the most harmful. In contrast, chronic strains are enduring problems, conflicts, and threats people face (Pearlin et al. 1981). In the context of hypertension in Black patients, perceived racism in health displays the convergence between chronic strains and life events. Racism is a chronic strain that many African Americans face through racial profiling, police brutality, discrimination, and other forms of bias (Powell et al. 2018).
Stress Process Theory and Medical Mistrust
The study found that in healthcare, the chronic strain of experienced racism may raise concerns about differential treatment based on race. Black men who were frequently exposed to racism were more likely to avoid blood pressure screening and routine health care visits. More frequent negative interactions with providers cause ‘wear and tear’ on Black patients’ trust in medical institutions (Powell et al. 2018).
Pearlin’s Stress Process Theory highlights how racism increases mistrust and lowers medical service utilization of Black patients. Therefore, for providers to improve medical adherence in Black HTN patients, they must improve their understanding of racism and its impacts on health outcomes.
Struggles to Implement Policy
With consideration of the existing literature on hypertension and the identified causes of poor adherence in Black patients, policymakers should implement policies that advocate for patients. Due to the nature of the policy issue, few policies have been passed to address the disparities in hypertension between Black and white patients. Policymakers have struggled to address medical mistrust, differential health outcomes, and poor medical adherence due to structural inequalities within health institutions. However, it is important to address that failures of policy action should not default blame on the individual.
Policy action is severely limited due to the extent of hypertension’s medicalization. Hypertension has been completely medicalized; as a result, the role of policy is constrained in patient-provider relationships (Mueller et al. 2014).
While the implementation of provider guidelines could be effective, it may be more to focus on how healthcare institutions and third parties can provide support, guidance, and resources for Black hypertensive patients with poor medical adherence.
Some suggestions include community-based interventions to address the lack of resources patients may have. African American patients “may be less likely to have strong social support, be educated about their medications, read prescription labels, and experience low medication costs” (Ferdinand et al. 2020).
A study by Dr. Carmen Alvarez emphasizes that nonadherence could not be combatted by social support alone, as it was with white patients. The unequal burden of hypertension highlights how differential treatment on the basis of race requires differential measures to combat systemic problems (Alvarez et al. 2021). Additionally, decreased access to continual and consistent care from a complete healthcare team contributes to lower medical adherence.
Existing Policy Solutions
1) Healthy Heart Community Prevention Project
The community-based intervention approach was utilized in 2000 by Daphne P. Ferdinand through a program called the Healthy Heart Community Prevention Project (HHCPP). HHCPP was a 12-month program that aimed to improve cardiovascular health outcomes by connecting communities to healthcare providers and volunteers. Through community gathering spaces like barber shops and churches, HHCPP aimed to educate high-risk individuals and provide resources to better control hypertension. Additionally, the program provides resources for providers who manage hypertensive patients (Ferdinand et al. 2020).
2) LA Blood Pressure Barrbershop Study
The LA Blood Pressure Barbershop (LABP) study employed a clinical pharmacist to conduct Hypertension medication therapy in 52 black-owned LA barber shops. The LABP successfully reduced both SBP and DBP and increased medical adherence.
The program allowed patients to have in-depth conversations about heart health, lifestyle changes, monitoring strategies, and medication regimens. The study provided patients with educational and practical resources to promote heart health, but it also began to mend relationships between Black communities and healthcare providers.
While policy actions may not have successfully addressed HTN in Black communities, policymakers can advocate for community-based approaches through funding and political advocacy (Ferdinand et al. 2020). Using the LABP Study as a model provides policymakers and community organizers with a framework to address medical nonadherence in Black hypertensive patients better and improve cardiovascular health outcomes in Black communities.
Policy Recommendations
Current measures do not address hypertension as a whole, prioritizing traditional biomedical approaches to treatment — i.e., medication regimens and lifestyle changes. After considering existing policy solutions, policymakers must utilize a multisectoral and multifaceted approach to address health outcomes and social determinants of health. The two approaches listed below explain how policymakers can combine both community-based and legal approaches to address hypertension in Black communities.
1) Community-Based Approach
The LABP study and HHCPP can be used as foundational frameworks for community- based approaches in hypertension management. As previously highlighted, external factors such as medical mistrust, lack of medical knowledge, and perceived racism in healthcare increase medical nonadherence. Community-based approaches use existing trust in community organizations and leaders to build trust between Black communities and healthcare providers and institutions. These programs have shown great promise in decreasing blood pressure levels and increasing adherence to medication regimens. Community-based programs are effective, but require collaboration from other sectors of healthcare to address all aspects of illness.
2) Revised Nondiscrimination Policy
As previously addressed, the patient-provider relationship is a critical factor in medical nonadherence in Black hypertensive patients. While community-based approaches tackle patient trust, policy can still improve the quality of patient experiences by revising nondiscrimination policy. The United States has two primary tools for anti-racist healthcare: Title VI of the Civil Rights Act of 1964 and Section 1557 of the Affordable Care Act (ACA).
Title VI of the Civil Rights Act “prohibit[s] discrimination based on race, color, or national origin in health care programs or other activities that receive federal funds or other federal financial assistance” (Allsbrook and Keith 2021). Recipients include “hospitals, health clinics, nursing homes, long-term care facilities, almost all physicians, and Medicaid and Medicare programs, among others” (Allsbrook and Keith 2021).
Since Title VI’s adoption in 1964, the political and social climate in the U.S. has shifted greatly. Originally intended to address blatant racism, Title VI is not equipped to handle more subtle forms of racism or de facto segregation. In 2010, the ACA built upon and extended the protections of Title VI (Allsbrook and Keith 2021). Section 1557 was written to address the gaps in Title VI, creating a new single health-specific, anti-discrimination cause of action that does not vary based on the patient’s protected class (that is, race, sex, disability, or age)” (Allsbrook and Keith 2021).
Although the scope of these policies is limited, they can act as a foundational framework for the future of nondiscrimination policy in healthcare. Potential changes include extending prohibition of discrimination to all physicians and recognizing a broader definition of discrimination (Allsbrook and Keith 2021). Further patient protections are needed to ensure that everyone receives the highest quality of care. To address the systemic and social determinants of medical nonadherence in Black hypertensive patients, policymakers must ensure that existing hard law has thorough protections in place.
Conclusion
In conclusion, policy action cannot successfully address medical nonadherence of Black hypertensive patients without addressing the systemic and structural contexts that place an unequal burden on African Americans in healthcare. Globally, Black Americans are the most vulnerable to hypertension, a major risk factor for cardiovascular disease and heart-related mortality and morbidities. Systemic issues such as racism continue to plague healthcare institutions, impacting access to services and mistrust in providers.
The focus on individualism must shift to a more holistic and community-centered approach. Providers must aim to rebuild community trust and strengthen communication and support. The issue of medical adherence in Black hypertensive patients requires a multisectoral and multifaceted response that addresses institutional barriers to care and the historical oppression of Black Americans in healthcare.
References:
Abel, Willie M., and Jimmy T. Efird. 2013. “The Association between Trust in Health Care Providers and Medication Adherence among Black Women with Hypertension.” Frontiers in Public Health 1. doi: 10.3389/fpubh.2013.00066.
Abel, Willie M., Telisa Spikes, and Danice B. Greer. 2021. “A Qualitative Study: Hypertension Stigma Among Black Women.” Journal of Cardiovascular Nursing 36(2):96. doi: 10.1097/JCN.0000000000000759.
AHA. 2024. “High Blood Pressure Among Black People.” Www.Heart.Org. Retrieved
December 3, 2024 (https://www.heart.org/en/health-topics/high-blood-pressure/know-your-risk-factors-for-high-blood-pressure/high-blood-pressure-among-black-people).
Allsbrook, Jamille Fields, and Katie Keith. n.d. “ACA Section 1557 As A Tool For Anti-Racist Health Care.” doi: 10.1377/forefront.20211207.962085.
Alvarez, Carmen, Anika L. Hines, Kathryn A. Carson, Nadia Andrade, Chidinma A. Ibe, Jill A. Marsteller, Lisa A. Cooper, and the RICH LIFE Project Investigators. 2021. “Association of Perceived Stress and Discrimination on Medication Adherence among Diverse Patients with Uncontrolled Hypertension.” Ethnicity & Disease 31(1):97. doi: 10.18865/ed.31.1.97.
Brown, Marie T., Jennifer Bussell, Suparna Dutta, Katherine Davis, Shelby Strong, and Suja Mathew. 2016. “Medication Adherence: Truth and Consequences.” The American Journal of the Medical Sciences 351(4):387–99. doi: 10.1016/j.amjms.2016.01.010.
Chobufo, Muchi Ditah, Vijay Gayam, Jean Soluny, Ebad U. Rahman, Sostanie Enoru, Joyce Bei Foryoung, Valirie N. Agbor, Alix Dufresne, and Tonga Nfor. 2020. “Prevalence and Control Rates of Hypertension in the USA: 2017–2018.” International Journal of Cardiology Hypertension 6:100044. doi: 10.1016/j.ijchy.2020.100044.
Cooper, Richard S., Katharina Wolf-Maier, Amy Luke, Adebowale Adeyemo, José R. Banegas, Terrence Forrester, Simona Giampaoli, Michel Joffres, Mika Kastarinen, Paola Primatesta, Birgitta Stegmayr, and Michael Thamm. 2005. “An International Comparative Study of Blood Pressure in Populations of European vs. African Descent.” BMC Medicine 3(1):2. doi:10.1186/1741-7015-3-2.
Ferdinand, Daphne P., Saihariharan Nedunchezhian, and Keith C. Ferdinand. 2020. “Hypertension in African Americans: Advances in Community Outreach and Public Health Approaches.” Progress in Cardiovascular Diseases 63(1):40–45. doi: 10.1016/j.pcad.2019.12.005.
Ferdinand, Keith C., Fortunato Fred Senatore, Helene Clayton-Jeter, Dennis R. Cryer, John C. Lewin, Samar A. Nasser, Mona Fiuzat, and Robert M. Califf. 2017. “Improving Medication Adherence in Cardiometabolic Disease: Practical and Regulatory Implications.” Journal of the American College of Cardiology. doi: 10.1016/j.jacc.2016.11.034.
Fiscella, Kevin, and Kathleen Holt. 2008. “Racial Disparity in Hypertension Control: Tallying the Death Toll.” Annals of Family Medicine 6(6):497. doi: 10.1370/afm.873.
Forouzanfar, Mohammad H., Patrick Liu, Gregory A. Roth, Marie Ng, Stan Biryukov, Laurie Marczak, Lily Alexander, Kara Estep, Kalkidan Hassen Abate, Tomi F. Akinyemiju, Raghib Ali, Nelson Alvis-Guzman, Peter Azzopardi, Amitava Banerjee, Till Bärnighausen, Arindam Basu, Tolesa Bekele, Derrick A. Bennett, Sibhatu Biadgilign, Ferrán Catalá-López, Valery L. Feigin, Joao C. Fernandes, Florian Fischer, Alemseged Aregay Gebru, Philimon Gona, Rajeev Gupta, Graeme J. Hankey, Jost B. Jonas, Suzanne E. Judd, Young-Ho Khang, Ardeshir Khosravi, Yun Jin Kim, Ruth W. Kimokoti, Yoshihiro Kokubo, Dhaval Kolte, Alan Lopez, Paulo A. Lotufo, Reza Malekzadeh, Yohannes Adama Melaku, George A. Mensah, Awoke Misganaw, Ali H. Mokdad, Andrew E. Moran, Haseeb Nawaz, Bruce Neal, Frida Namnyak Ngalesoni, Takayoshi Ohkubo, Farshad Pourmalek, Anwar Rafay, Rajesh Kumar Rai, David Rojas-Rueda, Uchechukwu K. Sampson, Itamar S. Santos, Monika Sawhney, Aletta E. Schutte, Sadaf G. Sepanlou, Girma Temam Shifa, Ivy Shiue, Bemnet Amare Tedla, Amanda G. Thrift, Marcello Tonelli, Thomas Truelsen, Nikolaos Tsilimparis, Kingsley Nnanna Ukwaja, Olalekan A. Uthman, Tommi Vasankari, Narayanaswamy Venketasubramanian, Vasiliy Victorovich Vlassov, Theo Vos, Ronny Westerman, Lijing L. Yan, Yuichiro Yano, Naohiro Yonemoto, Maysaa El Sayed Zaki, and Christopher J. L. Murray. 2017. “Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 Mm Hg, 1990-2015.” JAMA 317(2):165–82. doi: 10.1001/jama.2016.19043.
Fuchs, Flávio D. 2011. “Why Do Black Americans Have Higher Prevalence of Hypertension?” Hypertension 57(3):379–80. doi: 10.1161/HYPERTENSIONAHA.110.163196.
Link, Bruce G., and Jo C. Phelan. 2001. “Conceptualizing Stigma.” Annual Review of Sociology 27:363–85.
Lukoschek, Petra. 2003. “African Americans’ Beliefs and Attitudes Regarding Hypertension and Its Treatment: A Qualitative Study.” Journal of Health Care for the Poor and Underserved 14(4):566–87.
Mueller, Michael, Tanjala S. Purnell, George A. Mensah, and Lisa A. Cooper. 2015. “Reducing Racial and Ethnic Disparities in Hypertension Prevention and Control: What Will It Take to Translate Research into Practice and Policy?” American Journal of Hypertension 28(6):699–716. doi: 10.1093/ajh/hpu233.
Pearlin, Leonard I., Elizabeth G. Menaghan, Morton A. Lieberman, and Joseph T. Mullan. 1981. “The Stress Process.” Journal of Health and Social Behavior 22(4):337–56. doi: 10.2307/2136676.
Powell, Wizdom, Jennifer Richmond, Dinushika Mohottige, Irene Yen, Allison Joslyn, and Giselle Corbie-Smith. 2019. “Medical Mistrust, Racism, and Delays in Preventive Health Screening Among African-American Men.” Behavioral Medicine 45(2):102–17. doi: 10.1080/08964289.2019.1585327.
Roger Magnusson and Lawrence O. Gostin. 2023. “Non-Communicable Disease.” in Global Health Law & Policy. Oxford University Press.
WHO. 2024. “Hypertension.” (https://www.who.int/news-room/fact-sheets/detail/hypertension).