
Inclusive Medical Literature: Addressing Disparities in Healthcare

Dermatologist Jenna Lester, one of the leading professionals in researching medical literature and its lack of representation
Healthcare disparities between racial groups in the United States, despite being one of the most developed countries in the world, are ever-prevalent in the 21st century. Dermatologist Jenna Lester, one of the leading professionals in the field, recounts a time where a patient of color had a rash which was “subsequently diagnosed as toxic epidermal necrolysis,” but because of suboptimal care, the patient sat in the emergency room for hours. Why did the patient sit in the emergency room for hours despite the deadly rash on their arm? The patient did not have the “‘characteristic’ redness” that dermatologists rely on to make a diagnosis appear different on darker skin colors (Lester et al 2019). The experience of Lester is not uncommon, and in fact, because light skin is overrepresented in three out of four medical textbooks (Louie and Wilkes 2018) medical professionals are unable to treat diseases properly on people of color with darker skin tones. The 21st century has seen small developments in addressing this problem, as medical professionals have taken it into their own hands to create medical literature with a wide range of skin tones for diseases.
In a broader sphere, the disenfranchisement of people of color in the healthcare system makes it harder for these communities to receive proper medical care. The National Academy of Medicine found that black patients especially are less likely to receive proper care for medical issues even when other characteristics, such as insurance status, income, and age, are held constant (Bridges 2018). Race is a determining factor when it comes to medical care, and this can have really extreme implications for patients of color. It is a known fact that people of color are “more likely to die from cancer, heart disease, and diabetes” because of the color of their skin (Bridges 2018). In fact, “black people are 50% more likely to die from heart attacks or strokes than white people” (Lester et al 2019). Diseases, like diabetes, that can be properly managed if diagnosed and treated correctly are killing portions of the population because inadequate care. Therefore, people of color are left without members of their family, and communities of color become distrustful of the healthcare system. It becomes a vicious cycle in which people of color receive faulty medical care, face life-threatening repercussions, and communities of color are therefore left feeling that they will not receive proper medical care.
The duty of medical professionals is to treat patients to the fullest of their abilities. If this is the case, why are portions of the population not receiving the same medical care as other groups? The answer is two-fold. First, the healthcare system does not properly represent that communities it serves. In the field, 56% of physicians are white in comparison to 5% and 6% of physicians being Black (or African American) and Hispanic, respectively . If this is not shocking enough, 13% of the population identifies as Black and 19% of the population considers themselves Hispanic (“Cultural Diversity in Healthcare: USAHS” 2021). Therefore, there is a stark difference between the make-up of the healthcare system and that of the general population. Without proper representation in the medical field, it becomes clear why the medical care that people of color receive is lacking. There is not a proper understanding of the experience of people of color, so to have a physical of a different race creates a barrier to proper treatment. With the lack of medical literature representing diseases are darker skin tones, it really takes the eye of another person of color to treat the patient properly.
The second half to the dilemma in which people of color are not treated properly in the healthcare system is implicit racial bias. A study performed by Dayna Bowen Matthews found that implicit racial biases cause white physicians to improperly treat medical issues in people of color (Bridges 2018). This improper does not mean that the physician refuses to provide medical care. However, unconsciously, white physicians are more likely to provide less aggressive treatments for diseases like cancer and heart disease to black patients compared to white patients (Bridges 2018). More involved treatments are necessary for many types of diseases and can better the outcome for the patient. Implicit racial bias should be reason enough to work to make the healthcare system more racial inclusive. By increasing diversity in physicians and providing better medical literature, the healthcare disparities found among people of color compared to white people can start to diminish. There will be a greater understanding for the proper course of treatment for people of color and communities can start to heal.
Common Diseases found in People of Color
For the purposes of this article, it is important to focus on health disparities in relation to diseases of the skin. People of color are less likely to develop skin cancer, yet a review published by the American Academy of Dermatology has shown that people of color have a 70% rate of 5-year survival rates for melanoma while the white population has a 92% rate of survival. The three most common skin cancers found in people of color are squamous cell, basal cell, and melanoma cancer (Gupta et al 2016). In addition to skin cancer, common skin diseases found in people of color include sarcoidosis—which can cause organ damage if not identified properly—Erythema dyschromicum perstans, Cutaneous amyloid, and acne (Adelekun et al 2021). In the context of the COVID-19 Pandemic, the virus can cause a skin rash which can be used to identify the disease. People of color have experienced a death toll of double or more to white people due to COVID-19. More specifically, 1 in 555 Black Americans have died because of the virus which has been detrimental to this portion of the population (APM Research Lab Staff 2021). It is clear, therefore, that an early identification of this rash would be instrumental to slowly the death toll among people of color and allow for quick, proper treatment.
Melanoma found on darker skin (top image) compared to melanoma found on lighter skin tones (bottom image)


How do skin diseases appear on darker skin?
Skin diseases, although not all fatal, require proper treatment by medical professionals, and people of color constantly face mistreatment because doctors are unable to identify the disease. Without proper representation of people of color as physicians as well as a lack of medical literature in which diseases are presented on darker skin tones, communities of color are more than likely going to be subject to improper treatment. Patients with darker skin present symptoms differently than patients with light skin tones: “Dark skin can present with morphologic variants, subtle disease presentations, and disease manifestations require unique management and therapy” (Ebede and Papier 2006). It is crucial for dermatologists to be able to diagnose and treat skin conditions for people of color, but medical professionals often are unable to identify diseases because of the lack of representation in medical literature. Race should not be a determining factor when regarding medical treatment, and without a proper understanding of diseases and their presentation on darker skin, people of color are disproportionately exposed to improper treatment. Acne vulgaris, for example, tends to be more active than in people with lighter skin tones. Additionally, people of color can develop inflammatory papules and cysts which promote postinflammatory hyperpigmentation (dark spots), scarring, and keloids (Davis and Callender 2010). These diseases may not be fatal, but without proper treatment, they become a bigger problem than what would have been with a prompt diagnosis and treatment. In current times, COVID-19 affects the daily lives of everyone around the world, yet the disease has hit communities of color at higher rates. Specifically, black people comprise 13.4% of the United States population but made up more than 30% of COVID-19 cases. Since one of the symptoms to identify the disease is cutaneous manifestations, medical professionals need be able to identify and then diagnose COVID-19 to start proper treatment (Lester et al 2020).
Textbook Analysis: The Findings
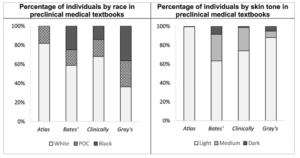
Several analyses of medical textbooks have been completed which indicate a bias against darker skin tones. In a study conducted by Patricia Louie and Rima Wilkes, the researchers analyzed 4146 images taken from the Atlas of Human Anatomy, Bate’s Guide to Physical Examination & History Taking, Clinically Oriented Anatomy, and Gray’s Anatomy for Students and coded race as well as skin tone at the textbook, chapter, and topic level. Gray’s was originally published in 1858 and is said to be “the world’s best-known medical book. Bates has been published since 1974, Atlas has been published since 1989, and Clinically has published since 1980. The problem of non-inclusive medical literature therefore has persisted since the 19th century and has made little progress. The analysis found that the textbooks did in fact approximate the distribution of races in the United States, but the skin tones — 74.5% light, 21% medium, 4.5% dark — show an overrepresentation of light skin tones. The proportion of dark skin tones found in all four of the textbooks were as follows: Atlas with 0.31%, Bates with 8.4%, Clinically with 1.1%, and Gray’s with 5%. In Clinically and Gray’s, 74.1% and 88.1% of individuals in the textbooks have light skin tones, respectively. In addition, there is an absence of people of color in numerous chapters (Louie and Wilkes 2018).
Left side: Distribution of Racial Representation Atlas, Bates’, Clinically, and Gray’s medical textbooks. Right side: Distribution of Skin Tones represented in Atlas, Bates’, Clinically, and Gray’s medical textbooks.
In a separate analysis carried out by Ademide Adelekun, Ginikanwan Onyekaba, and Jules B. Lipoff, the researchers found that general medical textbooks contain only 4.5% of images displaying dark skin. Sauer’s was the only textbook that “had a greater than 1% increase in representations of phototype V or VI [dark toned] skin.” Only half of the analyzed textbooks had a patient with dark skin with acne vulgaris, despite the prevalence in people of color. Diseases, such as erythema dyschromicum perstans, found in higher rates in people of color, were not represented well in medical literature, yet infectious diseases, like syphilis, are well-represented in each skin type (Adelekun et al 2021).
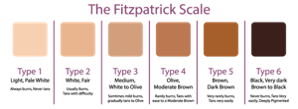
The Fitzpatrick scale of Skin Types is a numerical classification system for human skin color, developed in 1975 by American dermatologist Thomas B. Fitzpatrick.
Dermatologist Jenna Lester and her analysis of medical literature came when the COVID-19 pandemic began to ravage the United States, and she realized that there was a severe lack of representation of darker skin tones in images in medical literature (McFarling 2020). To carry out an analysis of this literature, Lester and her colleagues used 36 articles, with a total of 130 images. 92% of the images showed skin types I-III, the lightest on the Fitzpatrick skin tone spectrum, while only 6% of the images display type IV skin, a medium skin tone. In all of the images, there were none represented type V or VI skin, the darkest on the spectrum. In regards to race and ethnic background, 91% of patients were said to be white while the other 9% were Hispanic. The lack of representation for the darker skin tones, type V and VI, create a big problem for dermatologists because skin diseases, including that of COVID-19, present differently in people of color’s skin (Lester et al 2020). This analysis as well as the other two, above, are crucial for a full understanding of the disparities of darker skin tone representation found in common textbooks used by dermatologists (and medical professionals in general). It is clear that dermatologists, such as Jenna Lester, as well as professors of medicine, like Ademide Adelekun are taking it into their own hands to address this problem. The problem is not being addressed by textbook publishers, so the push by medical professionals is crucial. Without the work of these leading professionals, these undiversified resources will continue to be used, despite the severe implications they have on patients of color’s health.
A Problem Greater than just Textbooks: How the Lack of Diversity Affects Medical School Education
The top image includes examples of skin rashes associated with COVID-19. The bottom image shows an approximation of the skin tones represented in these images.

Through the various analyses of medical textbooks above, it is extremely clear that current medical literature, specifically medical literature commonly used in the dermatology field, is lacking in images of darker skin for even the most common of skin diseases. This problem, however, stems further from trained dermatologists: students in medical school are not being taught to the fullest potential because resources are lacking. Dr. Lynn McKinley-Grant, a professor of dermatology at Howard University states: “Often in medical schools, they have limited pictures in skin of people of color” (Prichep 2019). The implications of this are immense. Future doctors are being trained with resources not representative of the make-up of the population. Associate professor of dermatology at the University of Rochester, Dr. Art Papier, emphasizes the importance of pattern recognition in medical school classes. If pattern recognition is such an important aspect in medical training, especially for dermatology, then the lack of diversity in medical literature is an extremely prevalent problem. LaShyra Nolen, a first-year student at Harvard Medical School, recalls a time where her microbiology teacher could not answer how the “classic Lyme disease bull’s eye rash” presented on darker skin (Prichep 2019). In order for there to be any progress made in medical training, and in the dermatology field in general, in treating patients of color, there needs to be more diverse resources provided in the market. While there may not be many resources currently with greater representation of darker skin tones, progress is slowly being made.
The Work of Medical Student Malone Mukwende
The work of Malone Mukwende, a 20-year-old medical student at St. George’s University in London from Zimbabwe, in creating medical literature with more diverse skin representation highlights how disparities in medical resources are found in all parts of the world, not just the United States. Mukwende “noticed a lack of teaching about darker skin tones, and how certain symptoms appear differently in those who aren’t white” from the very start of his education at St. George’s (Page 2020). Having a darker skin himself, the medical student knew that symptoms for common skin diseases and physical reactions would appear different than on lighter skin, and not having resources representing darker skin tones would lead to incomplete education in medical schools and improper medical treatment for people of color. Mukwende took it upon himself to create “a universal tool” for people all around the world to be able to use (Page 2020).
With the help of senior lecturer Margot Turner, who is responsible for creating a more diverse curriculum, and Dr. Peter Tamony, Mukwende came up with the idea to write a book called Mind the Gap: A Handbook of Clinical Signs in Black and Brown Skin. Dr. Tamony knew that this book was extremely important, as he is aware that the school’s “methods of teaching were unfairly disadvantaging and ‘othering’ students from black and minority ethnic groups” (Page 2020). In addition, Tamony, Turner, and Mukwende understand that without proper educational materials,
medical students are not receiving the best education to treat people of color in the future. Mukwende points out that “if we don’t do anything about addressing the issue at hand, people will continue to be misdiagnosed” which can have dire consequences on the health of patients. The three began writing the book in December of 2019 (Page 2020). The book will include images of common clinical signs of diseases, like cancer and eczema, as well as suggest language for health-care workers to use “to decolonize the curriculum.” Mukwende expressed the challenge that they faced when compiling images of diseases with darker skin tones, as they are very lacking in medical resources. However, hours of persistence and research allowed them to create the book (Page 2020). Once this book goes into circulation, the hope is for medical schools as well as doctors from all around the world to put it into use, including the United States. With the work of Mukwende, the medical field is one step closer to providing the most effective treatment for people of color. Proper treatment means proper diagnosis. If doctors are able to identify diseases, like skin cancer, on patients of color, it stands to reason that the 70% survival rate of people of color—compared to 92% in white people—will rise significantly (Gupta et al 2016). Progress starts with the work of people like Malone Mukwende.
The cover of Muwende, Tamony, and Turner’s medical textbook Mind the Gap: A Handbook of Clinical Signs in Black and Brown Skin.
Progress in the Field: New Medical Literature
While Mind the Gap: A Handbook of Clinical Signs in Black and Brown Skin is an innovation in the progress of medical literature representation for darker skin tones, the Dermatology for Skin of Color is currently the main book used in the dermatology field. This book was first written by A. Paul Kelly and Susan C. Taylor in 2009, and since then has had two editions. The book emphasizes “distinct cutaneous disorders, reaction patterns, and cultural practices that all contribute to the clinical impression of people of color” (Kelly et al 2016). The book is organized in disease-specific chapters which first begin with a text box that summarizes key points such as “clinical features, pathogenesis, diagnostic tests, differential diagnoses, and treatment alternatives” (Sethi et al 2012). The book contains clinical photographs in each section for each disease, such as sarcoidosis, with varying skin tones in order to allow doctors to better identify diseases on patients of color. Specifically, each skin disease has at least two to three skin types represented in clinical images. The book has a unique feature not found in other medical resources (for skin of color): it contains a significant “variety of clinical images across a wide distribution of disease in a diverse population of people.” The textbook, therefore, not only represents a range of darker skin tones but also a range of ethnicities which do affect how diseases need to be treated (Sethi et al 2012).
The Implications of New Inclusive Literature
Dermatology for Skin of Color by Taylor et al. It is clear from the cover that the book contains images for skin disease on a range of skin tones
Historically, medical literature often used in the dermatology field has minimal focus on skin of color. With the ever-changing demographics and patient populations, specifically in increase of the population of color to about 47% of the population by the year 2060, it is crucial to develop resources for dermatologists to better treat patients of color (Kelly et al 2016). Developments in new, inclusive medical literature are crucial to the improvement of disparities in healthcare for people of color. It is clear that the lack of varying skin color in medical textbooks has greater effects on multiple aspects of society. Dermatologist Jenna Lester indicates that when there is a lack of confidence in diagnostic abilities in doctors, it affects “the physician-patient relationship” and leads to mistrust in the medical system in communities of color. In addition, those training to be dermatologists, who identify as people of color, become frustrated because they have to work in a system where “their race is overlooked or presented in a distorted way” (Lester et al 2019). Most importantly, it is evident that people of color face misdiagnosis and even higher death rates, in the case of melanoma, because doctors cannot identify and treat the diseases properly due to lack of exposure to diverse medical literature.
The two medical textbooks mentioned in the previous section are extremely important in making the field of dermatology more inclusive and in the long run decrease the disparities in healthcare for people of color. Progress is being made in other parts of the dermatology field. The Skin of Color Society, which was developed in 2004 by Dr. Susan C. Taylor, has become an important part of the National Medical Association, as it promotes the effect of skin color in dermatology. In addition, the American Academy of Dermatology continues to work to provide resources, like classes and new research, for dermatologists to better treat people of color (Adelekun et al 2021).
Wrapping up: What does this mean for society?
The experience of dermatologist Jenna Lester, in which a patient of color sat in the emergency room for hours despite having toxic epidermal necrolysis, should make it painfully clear that there is a problem in the current state of the field of dermatology. However, the blame cannot be put on the medical professionals, as without proper resources that include a range of skin tones, there is no way to know how a disease will present itself on darker skin tones. The current state of medical literature highlights the systemic racism ingrained in society against people of color. People of color are subjected to faulty medical treatment because there is improper representation of the population within medical resources. Without addressing the problem head-on by creating new resources, people of color will continue to be subjected to disparities in healthcare which has effects on death rates, disease prevalence, and even the perception of people of color from outside communities. The progress with the creation of more inclusive medical literature, such as Mind the Gap: A Handbook of Clinical Signs in Black and Brown Skin and Dermatology for Skin of Color, as well as the efforts of the Skin of Color Society are important stepping stones in decreasing the disparities of health in people of color.
Sources
Adelekun A, Onyekaba G, Lipoff JB. Skin color in dermatology textbooks: an updated evaluation and analysis. Journal of the American Academy of Dermatology. 2021;84(1):194–196. doi:10.1016/j.jaad.2020.04.084
APM Research Lab Staff. “Color of Coronavirus: Covid-19 Deaths Analyzed by Race and Ethnicity.” APM Research Lab, 5 Mar. 2021, https://www.apmresearchlab.org/covid/deaths-by-race.
Bridges, Khiara M. “Implicit Bias and Racial Disparities in Health Care.” Americanbar.org, American Bar Association , 1 Aug. 2018, https://www.americanbar.org/groups/crsj/publications/human_rights_magazine_home/the-state-of-healthcare-in-the-united-states/racial-disparities-in-health-care/.
“Cultural Diversity in Healthcare: USAHS.” University of St. Augustine for Health Sciences, University of St. Augustine, 16 Nov. 2021, https://www.usa.edu/blog/diversity-in-healthcare/.
Davis EC, Callender VD. A review of acne in ethnic skin: pathogenesis, clinical manifestations, and management strategies. ResearchGate. 2010 Apr 3 [accessed 2021 Apr 26]. https://www.researchgate.net/publication/45721887_A_review_of_acne_in_ethnic_skin_Pathogenesis_clinical_manifestations_and_management_strategies.
Ebede T, Papier A. Disparities in dermatology educational resources. Journal of the American Academy of Dermatology. 2006;55(4):687–690. doi:10.1016/j.jaad.2005.10.068
Gupta AK, Bharadwaj M, Mehrotra R. Skin cancer concerns in people of color: risk factors and prevention. Asian Pacific journal of cancer prevention : APJCP. 2016 [accessed 2021 Apr 26]. https://pubmed.ncbi.nlm.nih.gov/28125871/.
Jackson BA. Skin cancer in skin of color. Skin Cancer Management. 2009:217–223. doi:10.1007/978-0-387-88495-0_16
Kelly AP, Taylor SC, Lim HW, Maria ASA. Taylor and Kelly’s dermatology for skin of color. New York, NY: McGraw-Hill Education; 2016.
Lester JC, Jia JL, Zhang L, Okoye GA, Linos E. Absence of images of skin of colour in publications of COVID‐19 skin manifestations. British Journal of Dermatology. 2020;183(3):593–595. doi:10.1111/bjd.19258
Lester JC, Taylor SC, Chren MM. Under‐representation of skin of colour in dermatology images: not just an educational issue. British Journal of Dermatology. 2019;180(6):1521–1522. doi:10.1111/bjd.17608
Louie P, Wilkes R. Representations of race and skin tone in medical textbook imagery. Social Science & Medicine. 2018;202:38–42. doi:10.1016/j.socscimed.2018.02.023
McFarling UL, Jean B, Smith G, Fotsch E. Lack of darker skin in textbooks, journals harms patients of color. STAT. 2020 Jul 20 [accessed 2021 Apr 13]. https://www.statnews.com/2020/07/21/dermatology-faces-reckoning-lack-of-darker-skin-in-textbooks-journals-harms-patients-of-color/.
Page S. A medical student couldn’t find how symptoms look on darker skin. He decided to publish a book about it. The Washington Post. 2020 Jul 22 [accessed 2021 Apr 13]. https://www.washingtonpost.com/lifestyle/2020/07/22/malone-mukwende-medical-handbook/.
Sethi A, Francis S, Finch TV. Dermatology for skin of color, 1st ed. Journal of the American Academy of Dermatology. 2012;67(1). doi:10.1016/j.jaad.2010.05.018